This TSAB Falls and Safeguarding Guidance has been developed to support staff in making decisions about when to raise a safeguarding concern in relation to falls.
The toolkit has been developed by a multi-agency task and finish group and in consultation with relevant service providers.
We gratefully acknowledge the agreement of both North Tyneside Safeguarding Adults Board and Newcastle Safeguarding Adults Board in using some of their materials.
Safeguarding adults is protecting an adult’s right to live in safety, free from abuse and neglect. It is about people and organisations working together to prevent and stop abuse and neglect happening [1].
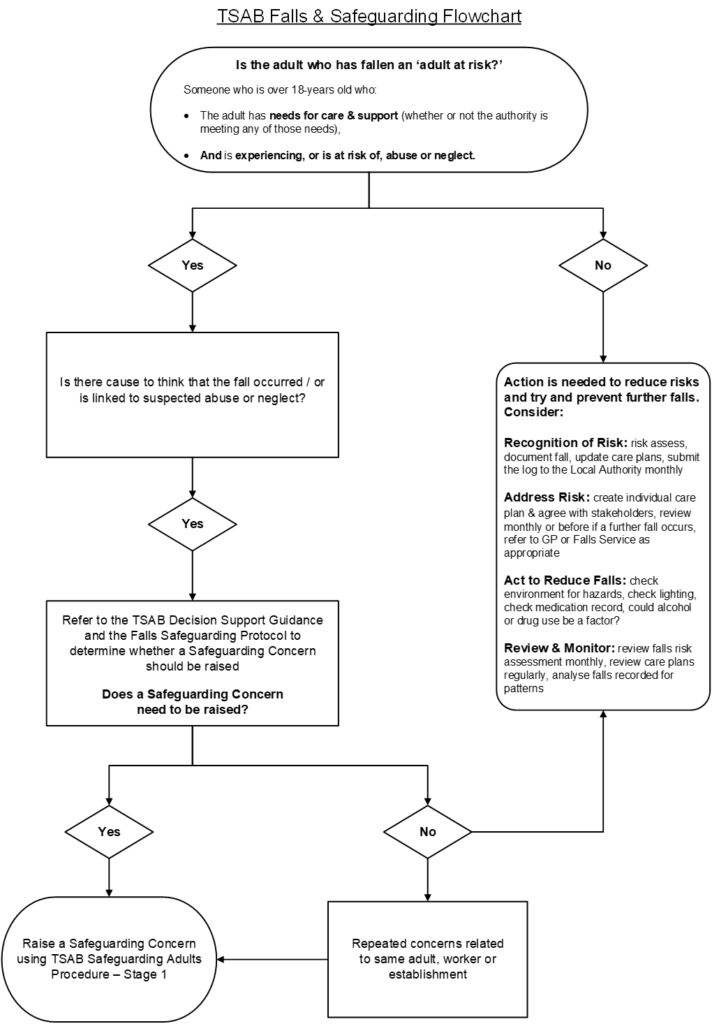
Safeguarding duties apply to adults over 18 years old and:
- have care and support needs (whether or not the Local Authority is meeting any of those needs)
- is experiencing, or at risk of, abuse and neglect
An adult at risk may therefore be a person who, for example:
- is an older person who is frail due to ill health, physical disability, or cognitive impairment
- has a learning disability
- has a physical disability and/or sensory impairment
- has mental health needs including dementia
- has a long-term illness/condition
- misuses substances or alcohol
- is an unpaid carer, such as a family member/ friend who provides personal assistance
The Care and Support Guidance (2022) states that abuse and neglect can take place in many forms. In relation to falls this may be:
- Neglect and acts of omission
- Organisational abuse
- Physical abuse
- Self-Neglect
[1] Care and Support Statutory Guidance, 2022
Falls can significantly damage self-confidence, increase social isolation, reduce independence, and hasten a move into a residential care setting. The fear of falling may lead to deterioration in a person’s well-being and quality of life, even if the fall itself does not result in a serious consequence.
There is evidence that residents and service users are particularly at risk from falls and fractures in the first few months after admission to a new setting. This may be due to the environmental changes and/or a period of ill health prior to admission. It is therefore essential that all individuals are assessed for their risk of falling and a care plan put into place to manage risk, prior to, or as soon as possible after moving into residential care or a supported living environment.
Falls prevention strategies and interventions need to consider the fact that falls can have a number of causes, such as frailty, infection, confusion, and the effects of some prescribed drugs that require many different interventions.
Providers of health and care services will have a Falls Policy and Procedure; these should follow national guidance and good practice.
Please refer to Section 11 for further information and useful resources.
It is important to note the difference between an ‘unwitnessed fall’ and an ‘unexplained injury’.
An Unwitnessed fall is when a fall has occurred, and the person has explained what happened. If there is no suggestion that the fall occurred due to possible abuse, neglect or omission of care, a safeguarding concern is not required. All falls should continue to be reported in line with the service provider’s management of incidents policies, and contractual/registration requirements, with risk assessments being reviewed and post fall protocols being adhered to, whether a safeguarding concern is raised or not.
Any fall that is deemed as unwitnessed, unexplained and results in injury should be referred to as an unexplained injury, rather than an unwitnessed fall. In these circumstances the senior staff member on duty should use judgement based on the evidence available to determine what may have happened. If the person has an injury which cannot be explained, then this should be referred as a safeguarding concern.
In any event, it is important that immediate medical attention is sought when a person presents with any head injury whether or not the cause is known. If there are no injuries evident at the time of the incident, ongoing monitoring must be undertaken, and advice sought if there is any change to clinical presentation.
Remember:
- Not all falls will require a safeguarding concern to be raised.
- The person raising the safeguarding concern will need to consider whether the person is an adult at risk and whether there was abuse or neglect linked to the fall.
- A safeguarding concern is not the route to access further support/ services in relation to falls.
What to consider:
A fall can be a safeguarding concern if there is abuse or neglect linked to it. There could be concerns that the fall occurred because of abuse or neglect (including self-neglect) or that care and treatment following a fall was abusive or neglectful.
The person raising the safeguarding concern will need to decide whether one of the following categories of abuse apply:
- Neglect – the person/s responsible for the care and support needs (whether paid or unpaid) did not carry out their responsibilities as expected before or after the fall
- Organisational abuse – the fall occurred because of wider systemic failures within an organisation e.g. failure to carry out risk assessments, poor staffing levels, lack of communication regarding care plan
- Physical abuse – someone pushed or tripped the adult resulting in the fall
- Self-neglect – the fall happening because of a lack of self-care, care of the environment or a refusal of services. Mental capacity will be a key consideration in these cases.
The following questions might be helpful in determining whether the fall should be referred as a safeguarding concern.
Once a decision has been made to raise a safeguarding concern, it is important that the normal referral routes are used. This may be directly into the Local Authority or via the organisation’s safeguarding adults team or lead. Please see TSAB Inter-agency Safeguarding Adults Procedures. If wilful neglect or any other criminal act is suspected, then the police must be contacted.
Specific information which should be included in the Safeguarding Concern form includes:
- Any injuries sustained as a result of the fall (attach body map to the concern)
- Information relating to previous falls/ falls risk/ falls risk assessment
- Action taken following the fall (e.g. medical intervention, contact with the person and their family)
- Any plans put in place to address an increased risk in falls
There is an expectation that safeguarding concerns are discussed with the individual and/or their representative wherever possible, and that they are involved in discussing the concern and agreeing on an appropriate course of action. This is called Making Safeguarding Personal (MSP). In cases where there is a pattern of falls involving one or more people receiving care from the same provider, a safeguarding concern will need to be raised even if the person is not in agreement in order to safeguard others who use the service.
If the fall does not require a safeguarding adults concern to be raised, there will be actions that need to be considered to reduce risks and to try and prevent falls happening again in the future. It is also good practice to record the rationale for not raising a safeguarding concern.
Recognition of Risk
- Assessment of risk prior to commencing service
- Complete falls risk assessment
- Document falls history
- Ensure all falls are recorded on the incident form or log for further analysis
- Update Care Plans
- Submit the log to the Local Authority each month
Address risk
- Write individual care plan to cover risks to service user/ patient
- Agree care plan and sign off by all stakeholders
- Review monthly or before this if a further fall occurs
- Provide falls prevention information
- Refer to GP or Falls Service, as appropriate
Act to reduce falls
- Check environment for trip/slip hazards, including the condition of carpets and uneven floor surfaces
- Check lighting is sufficient/ have eye tests been carried out recently
- Is the medication record up to date
- Could alcohol/ drug use be a factor?
Review and monitor
- Review falls risk assessment monthly or if there are changes to medication, physical or mental health or if a fall occurs
- Review care plan if there are changes to medication, health or falls
- Analyse falls recorded on the incident /accident logs for triggers or patterns. Multiple falls related to the same person and/ or service might suggest the need for a safeguarding concern to be raised.
On receipt of the safeguarding adults concern, the Local Authority will decide whether there is a duty to conduct a Safeguarding Adults Enquiry (Section 42) to investigate the concern. The Local Authority may carry out the enquiry themselves or may determine that they are able to ‘cause’ the enquiry to be undertaken by someone else, for example, the provider. Please see Causing Section 42 Enquiries Guidance.
Whoever is undertaking the enquiry should consider who should be involved; the list below is not exhaustive and it will depend on the circumstances of the concern.
- The person/ representative
- The Local Authority Safeguarding Team (should be involved in all cases where the concern relates to a paid worker, volunteer or service provider)
- Falls specialists
- Service Provider (health, social care, housing)
- CQC
- Commissioner
- Community team and rehabilitation team
- Community nurse
- Social worker
- Police
- Coroner (in the event of death)
- Health and Safety Executive
The following list provides some examples of actions that may feature in a safeguarding adults plan where the concern relates to falls.
- Holistic falls risk assessment
- Multiple Interventions for example: physical health, mental health and emotional needs
- Referral to Falls Clinic
- Medical/ care needs assessment
- Home hazard’s assessment and safety interventions
- Provision of equipment or aids
- Training for staff
- Revision of policy and procedures
- Disciplinary action (including possible referral to DBS/ professional bodies)
- Criminal action
- Care Act 2014
- Department of Health & Social Care (2014) Care and Support Statutory Guidance
- National Institute for Excellence (2013) Falls in older people
- National Institute for Excellence (2015) Preventing falls in care homes
- National Institute for Health and care Excellence (2013) Preventing falls in care homes
Version Control:
June 2024 – Version 1.3